Multifocal Atrial Tachycardia
What Is MAT?
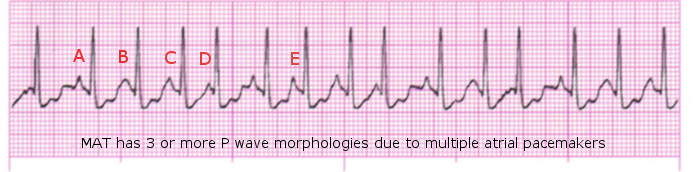
Multifocal Atrial Tachycardia (MAT) can be seen in acutely ill patients with significant pulmonary disease is seen in about 60 percent of these patients. Some medications used to treat lung disease may exacerbate the dysrhythmia. Three different P waves are seen, indicating the electrical impulse is coming from more areas than just the SA node. (Source 1).
What Causes MAT?
MAT is caused by a number of conditions including but not limited to: lung disease including asthma, congestive heart failure, myocardial infarction, pnuemonia, and hypokalemia. (Source 2) Other factors include age (those over 50 have a greater risk of MAT), recent surgury, diabetes, and and overdose on Theophylline. (Source 5).
Symptoms
Symptoms of MAT include, but are not limited to: heart palpitations, lightheadedness, syncopal episodes, shortness of breath, and chest pain. (Source 5, Source 2).
Physical Findings
Physical findings of MAT include, but are not limited to: a rapid and irregular pulse (Source 2), possible signs of shock, including low blood pressure. A normal blood pressure, however, may be seen as well. (Source 5).
Complications
Multifocal Atrial Tachycardia may be confused with atrial fibrillation or atrial flutter, and may or may not cause an instable blood pressure. (Source 2).
EKG Findings
On an EKG, you will see a narrow-complex tachycardia with multiple morphologies of the P-wave. You may have varying P-R intervals and P-P intervals as well. (Source 4).
Treatment
Treatment of MAT includes treating the underlying cause first (See "What Causes MAT?") Further treatments include oxygen therapy to reverse ischemia, administering IV Magnesium, stopping medications including Theophylline that may increase heart rate, or heart-rate controlling medications including Verapamil or Diltiazem; or other selective beta blockers.
Group members
- Sara Loggin
- Jason Olds
- Pat Quimby
Sources
- Brady Paramedic Care, Principles & Practice; Medical Emergencies, Volume 3; Page 107
- Hemphill, Robin R. MD, MPH; eMedicine website article; "Multifocal Atrial Tachycardia"
- RnCeus.com; "Multifocal Atrial Tachycardia"
- Wikipedia page "Multifocal Atrial Tachycardia"
- New York Times, Health Guide; "Multifocal Atrial Tachycardia"